Time to benefit: How Long Will It Take for a Test or Treatment to Help Your Patient
Time to benefit is the time between the intervention (usually a test or treatment) and its benefit.
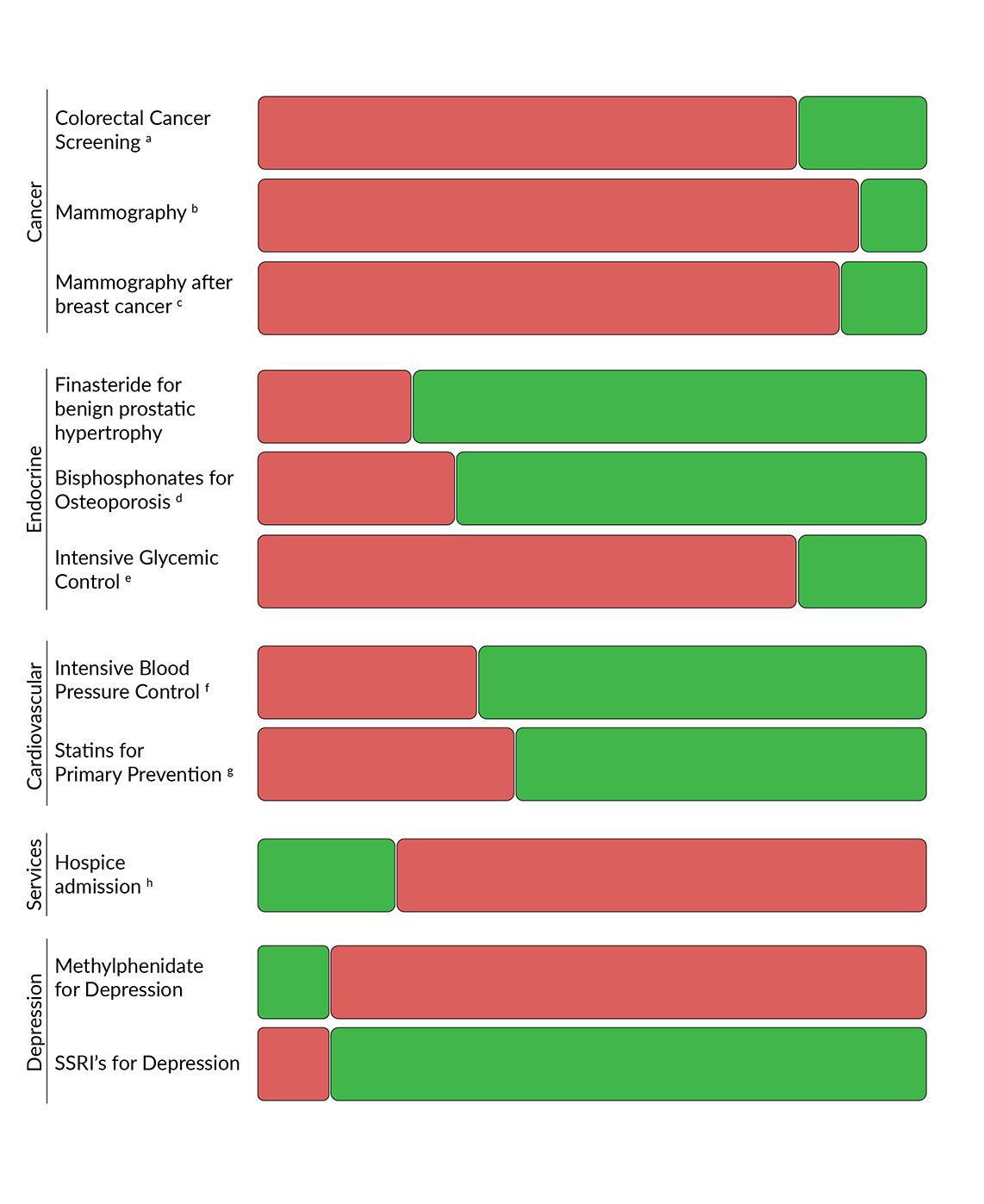
The following figure shows which preventive treatments your patient may benefit from and which may be harmful based on your patient’s life expectancy and the time to benefit for each intervention. If time to benefit is longer than the patient's life expectancy, then the patient is unlikely to benefit from the intervention. If time to benefit is shorter than the patient's life expectancy, then the patient is likely to benefit from the intervention.
 Generally recommended
Generally recommended
 Generally not recommended
Generally not recommended
- To prevent death from colorectal cancer
- To prevent death from breast cancer.
- To prevent death from breast cancer for most women with history of breast cancer. See citations below for exceptions.
- To prevent a nonvertebral fracture
- Blood HbA1C range < 7%. To prevent dialysis and retinopathy (<8 years for most patients). The guideline is primarily supported by the United Kingdom Prospective Diabetes Study (UKPDS)
- Systolic blood pressure <140 mmHg to prevent major adverse cardiovascular events including death.
- To prevent major cardiovascular events. The data for statin benefit for primary prevention is limited for patients over age 75
- The 6-month estimate is more driven by policy than evidence, it may be beneficial for even longer life expectancies
Time to Benefit Citations:
Cancer:
Time lag to benefit after screening for breast and colorectal cancer: meta-analysis of survival data from the United States, Sweden, United Kingdom, and Denmark.
Lee SJ, Boscardin WJ, Stijacic-Cenzer I, Conell-Price J, O'Brien S, Walter LC.
BMJ. 2013 Jan 8;346:e8441. doi: 10.1136/bmj.e8441. PMID: 23299842
Time to benefit for colorectal cancer screening: survival meta-analysis of flexible sigmoidoscopy trials.
Tang V, Boscardin WJ, Stijacic-Cenzer I, Lee SJ.
BMJ. 2015 Apr 16;350:h1662. doi: 10.1136/bmj.h1662. Erratum in: BMJ. 2015;350:h2228.
PMID: 25881903
Screening for Colorectal Cancer in Asymptomatic Average-Risk Adults: A Guidance Statement From the American College of Physicians (ACP)
Amir Qaseem, Carolyn J. Crandall, Reem A. Mustafa, Lauri A. Hicks, and Timothy J. Wilt
Annals of Internal Medicine 2019 171:9, 643-654
Screening for Breast Cancer in Average-Risk Women: A Guidance Statement From the American College of Physicians (ACP)
Amir Qaseem, Jennifer S. Lin, Reem A. Mustafa, Carrie A. Horwitch, and Timothy J. Wilt
Annals of Internal Medicine 2019 170:8, 547-560
Freedman RA, Minami CA, Winer EP, et al. Individualizing Surveillance Mammography for Older Patients After Treatment for Early-Stage Breast Cancer: Multidisciplinary Expert Panel and International Society of Geriatric Oncology Consensus Statement. JAMA Oncol. Published online January 28, 2021.
doi:10.1001/jamaoncol.2020.7582
Endocrine:
Gormley GJ, Stoner E, Bruskewitz RC, Imperato-McGinley J, Walsh PC, McConnell JD, Andriole GL, Geller J, Bracken BR, Tenover JS, et al. The effect of finasteride in men with benign prostatic hyperplasia. The Finasteride Study Group. N Engl J Med. 1992 Oct 22;327(17):1185-91. doi: 10.1056/NEJM199210223271701. PMID: 1383816.
King P, Peacock I, Donnelly R. The UK prospective diabetes study (UKPDS): clinical and therapeutic implications for type 2 diabetes. Br J Clin Pharmacol.
1999;48(5):643-648. doi:10.1046/j.1365-2125.1999.00092.x
Estimating the Time to Benefit for Preventive Drugs with the Statistical Process Control Method: An Example with Alendronate. van de Glind EM, Willems HC, Eslami S, et al. Drugs Aging. 2016;33(5):347-353. doi:10.1007/s40266-016-0344-7
Deardorff WJ, Cenzer I, Nguyen B, Lee SJ. Time to Benefit of Bisphosphonate Therapy for the Prevention of Fractures Among Postmenopausal Women With Osteoporosis: A Meta-analysis of Randomized Clinical Trials. JAMA Intern Med. Published online November 22, 2021. doi:10.1001/jamainternmed.2021.6745
Cardiovasular:
Rationalizing prescribing for older patients with multimorbidity: considering time to benefit.
Holmes HM, Min LC, Yee M, Varadhan R, Basran J, Dale W, Boyd CM.
Drugs Aging. 2013 Sep;30(9):655-66. doi: 10.1007/s40266-013-0095-7. Review.
PMID: 23749475
Pharmacologic Treatment of Hypertension in Adults Aged 60 Years or Older to Higher Versus Lower Blood Pressure Targets: A Clinical Practice Guideline From the American College of Physicians and the American Academy of Family Physicians
Amir Qaseem, Timothy J. Wilt, Robert Rich, Linda L. Humphrey, Jennifer Frost, and Mary Ann Forciea
Annals of Internal Medicine 2017 166:6, 430-437
Yourman LC, Cenzer IS, Boscardin WJ, et al. Evaluation of Time to Benefit of Statins for the Primary Prevention of Cardiovascular Events in Adults Aged 50 to 75 Years: A Meta-analysis. JAMA Intern Med. 2021;181(2):179–185. doi:10.1001/jamainternmed.2020.6084
Chen T, Shao F, Chen K, et al. Time to Clinical Benefit of Intensive Blood Pressure Lowering in Patients 60 Years and Older With Hypertension: A Secondary Analysis of Randomized Clinical Trials. JAMA Intern Med. Published online May 09, 2022. doi:10.1001/jamainternmed.2022.1657
Services:
Hospice. Centers for Medicare and Medicaid. Updated December 12, 2021. Accessed February 15, 2022
Luchins, D.J., Hanrahan, P. and Murphy, K. (1997), Criteria for Enrolling Dementia Patients in Hospice. Journal of the American Geriatrics Society, 45: 1054-1059
Depression:
Widera EW, Block SD. Managing grief and depression at the end of life. Am Fam Physician. 2012 Aug 1;86(3):259-64. PMID: 22962989
Meghan Ellinger May, Amy VandenBerg; The role of methylphenidate in depression. Mental Health Clinician 1 November 2015; 5 (6): 271–276. doi: 10.9740/mhc.2015.11.271
DISCLAIMERThe information provided on ePrognosis is designed to complement, not replace, the relationship between a patient and his/her own medical providers. ePrognosis was created with the support of the Division of Geriatrics at the University of California San Francisco. However, its content is strictly the work of its authors and has no affiliation with any organization or institution. This web site does not accept advertisements. If you reproduce the material on the website please cite appropriately. For feedback and questions regarding the site please email Sei Lee, MD (sei.lee@ucsf.edu), Alex Smith, MD (aksmith@ucsf.edu) or Eric Widera, MD (eric.widera@ucsf.edu).