1. Why isn't there a calculator that estimates life expectancy?
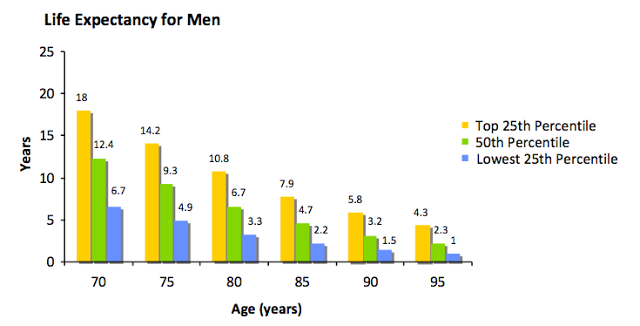
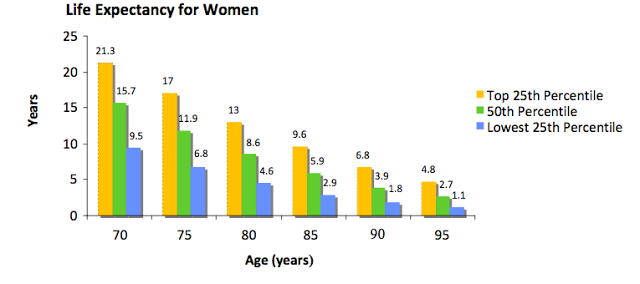
As far as we know, no such calculator exists. However, life expectancy estimates generated by US census data are one method of obtaining this information (see Figure below). However, clinicians must first decide if their patient falls in the upper 25th percentile, middle 50th percentile, or lowest 25th percentiles for their age group. The prognostic indices in the ePrognosis compendium may assist with this determination. Using multiple sources may improve the accuracy of the prognostic estimate. Keeler and colleagues improved upon the life-table method by including mobility-impairment and activities of daily living (ADL)-impairment. This method has not been validated, however. When used in conjunction with a prognostic index, the information from life tables may be a useful additional source of information.
2. Why isn't there just one calculator? Why all the different calculators?
It is not possible to develop a life expectancy calculator that is accurate for everybody and all situations. For example, a life expectancy calculator may be accurate for 50 year olds, but much less accurate for 90 year olds; a mortality prediction index may work great for predicting 1 year mortality but not for predicting 10 year mortality. Thus, to be able to predict life expectancy accurately for all older adults over a wide range of time frames, numerous mortality indices have been developed so that providers will be able to choose the life expectancy calculator that is most appropriate for any given older patient and clinical situation. We hope that by compiling and organizing mortality indices, we can help busy clinicians choose and use the most appropriate mortality indices for their patients.
3. If my patient modifies one of the factors on the index, such as smoking, does his or her risk change to the modified level?
Not necessarily. These indices were created to predict risk, not evaluate changes in risk due to risk factor modification. Take a patient who currently smokes and has a score of 10 and 20-28% risk of dying in 4 years. A similar patient who reports not being a current smoker would have a risk score of 8 and a 15-20% 4 year mortality. However, it is not clear if the risks for a person who stops smoking today are the same as the risks for a person who never smoked.
Furthermore, these studies found risk factors for mortality. These risk factors may have no true causal association with mortality. For example, people who carry matches may be at increased risk for mortality, and matches may end up in the prognostic index. These people are at risk for dying not because they carry matches, however, but because they carry matches to light cigarettes. By not carrying matches, but continuing to smoke, these people would do nothing to change their risk of death.
